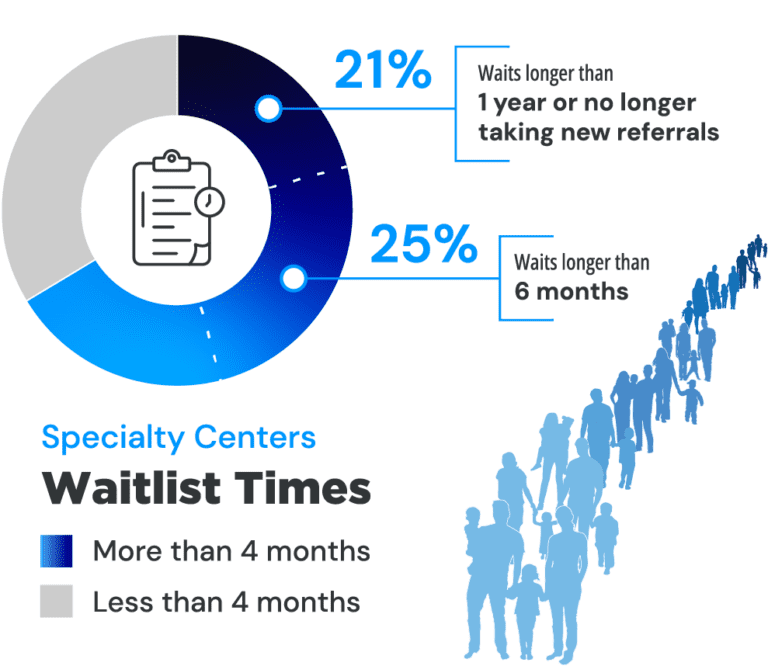
A new analysis of specialty centers across the U.S. confirms that families concerned about their child’s development and behavioral health face unacceptably long wait times, unnecessarily complex and highly variable processes, and reimbursement barriers and inequities – all adding up to delayed diagnosis and missed opportunities for life-changing early intervention for children.
A new analysis of specialty centers across the U.S. confirms that families concerned about their child’s development and behavioral health face unacceptably long wait times, unnecessarily complex and highly variable processes, and reimbursement barriers and inequities – all adding up to delayed diagnosis and missed opportunities for life-changing early intervention for children.
An analysis of 111 specialty centers in the U.S. confirms the crisis of care for children and families seeking a diagnosis of developmental delays and autism evaluation. The delays in diagnosis revealed by this survey demonstrate why many children with autism, and other developmental/behavioral conditions, are missing a critical early intervention period when significant, positive impacts on neurological development can be made. This report of the survey’s key findings sheds light on the inequities and inefficiencies in the system that are leaving many children and families behind. The survey was designed and conducted by Scott Badesch, Former President of the Autism Society of America, and sponsored by Cognoa.
 A recent poll at the Society for Developmental & Behavioral Pediatrics Annual Meeting in September 2023 showed even longer wait lists. More than half of the audience of developmental behavioral pediatricians of academic or hospital affiliated centers self-reported waitlists of longer than 9 months.
A recent poll at the Society for Developmental & Behavioral Pediatrics Annual Meeting in September 2023 showed even longer wait lists. More than half of the audience of developmental behavioral pediatricians of academic or hospital affiliated centers self-reported waitlists of longer than 9 months.
Not enough specialists for the number of children in need
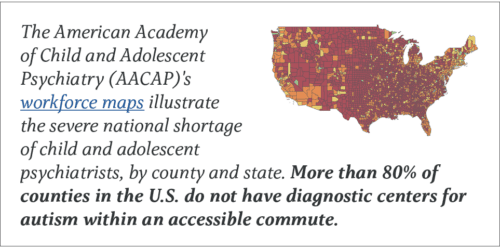
The volume of children needing evaluation exceeds the limited number of specialists who complete them. More than two-thirds of centers (69%) report shortages in their workforce. 61% percent of centers also report that volume of children referred to them is a barrier to making evaluations in a reasonable time frame.

* AAP
** 20% of CAPs are above age 70
*** AACAP
 “Primary care clinicians, specifically pediatricians, who are equipped with a diagnostic that is made for their setting can accurately and rapidly evaluate, diagnose, and manage most children with developmental delays and autism – all from within the medical home,” said Dr. Sharief Taraman, CEO of Cognoa, Past President of the American Academy of Pediatrics-Orange County Chapter and Board Member of the American Academy of Pediatrics-California, Associate Professor University of California-Irvine School of Medicine. “Yet, in most cases, the forces that be, be it tradition or policy, make the ‘autism specialist’ the only option for a diagnosis. This isn’t working for families, specialists, nor primary care clinicians. This is an imbalance that healthcare leaders and policymakers must take seriously when directing future resources and developing initiatives to standardize, equitize, and streamline evaluation processes for families, irrespective of insurance type. We as a nation are failing our children. It is vital that we expand and empower the pool of providers who can evaluate and diagnose children, and we need to start in primary care.”
“Primary care clinicians, specifically pediatricians, who are equipped with a diagnostic that is made for their setting can accurately and rapidly evaluate, diagnose, and manage most children with developmental delays and autism – all from within the medical home,” said Dr. Sharief Taraman, CEO of Cognoa, Past President of the American Academy of Pediatrics-Orange County Chapter and Board Member of the American Academy of Pediatrics-California, Associate Professor University of California-Irvine School of Medicine. “Yet, in most cases, the forces that be, be it tradition or policy, make the ‘autism specialist’ the only option for a diagnosis. This isn’t working for families, specialists, nor primary care clinicians. This is an imbalance that healthcare leaders and policymakers must take seriously when directing future resources and developing initiatives to standardize, equitize, and streamline evaluation processes for families, irrespective of insurance type. We as a nation are failing our children. It is vital that we expand and empower the pool of providers who can evaluate and diagnose children, and we need to start in primary care.”
The urgent need to engage the broader primary care workforce in the process of autism diagnosis is also recognized by the leadership of the American Academy of Pediatrics. Amongst AAP’s most recent top leadership resolutions is their commitment to take action to ensure a diagnosis of autism by pediatricians “allows the coverage of appropriate services by both private insurers and state Medicaid programs.”
Unnecessarily complicated & time-consuming processes
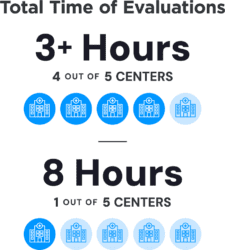 Another obstacle that limits access to a timely diagnosis is the lengthy evaluations that are routinely given irrespective of the complexity of their presentation. Multidisciplinary team assessments have created barriers because they are time-intensive, specialist dependent, hard to access, and expensive. In more than 4 out of 5 centers (83%), evaluations take more than three hours. One of every four specialty centers report that their evaluations can take 8 hours.
Another obstacle that limits access to a timely diagnosis is the lengthy evaluations that are routinely given irrespective of the complexity of their presentation. Multidisciplinary team assessments have created barriers because they are time-intensive, specialist dependent, hard to access, and expensive. In more than 4 out of 5 centers (83%), evaluations take more than three hours. One of every four specialty centers report that their evaluations can take 8 hours.
“Wait times, prolonged report writing time, and efficiency in the intake process are all real challenges in the diagnosis of children and adults with autism,” said another clinician in the survey. “A number of these challenges are perpetuated by professionals who continue to provide extensive evaluations that often duplicate those that have been completed within the school system and early intervention programs.”
Another clinician pointed out that the documentation requirements of autism assessment is a barrier for families: “The ability to complete all the documentation varies from family to family, and depends on their ability to complete forms, respond to calls, provide transportation, and be flexible with scheduling. Unfortunately, many families are not able to complete all the items needed.”
Barriers to reimbursement shut out the already disadvantaged
“Insurance companies create barriers to diagnosing efficiently,” said one provider in the survey. “One way they do this is by mandating specific measures that have known biases and disparities.”
 Families struggle to find ways to pay for lengthy autism assessments. The healthcare providers who provide developmental and autism assessments are not always covered by a family’s medical insurance. In these cases, families must either pay out of pocket and/or travel long distances.
Families struggle to find ways to pay for lengthy autism assessments. The healthcare providers who provide developmental and autism assessments are not always covered by a family’s medical insurance. In these cases, families must either pay out of pocket and/or travel long distances.
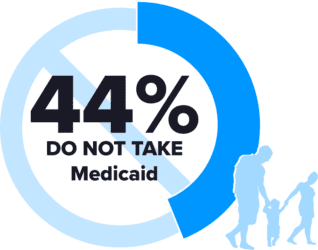
Disadvantaged families are affected the most, as 44% of centers surveyed do not take Medicaid, forcing families to find other ways to pay or forego assessment. Meanwhile, only 65% of practices take commercial insurance, so if families cannot pay costs out of pocket up front, there is a high likelihood they will be left behind altogether.